
Apocrine Cysts
Breast Core Needle Biopsy: Differential of Cystic Lesions

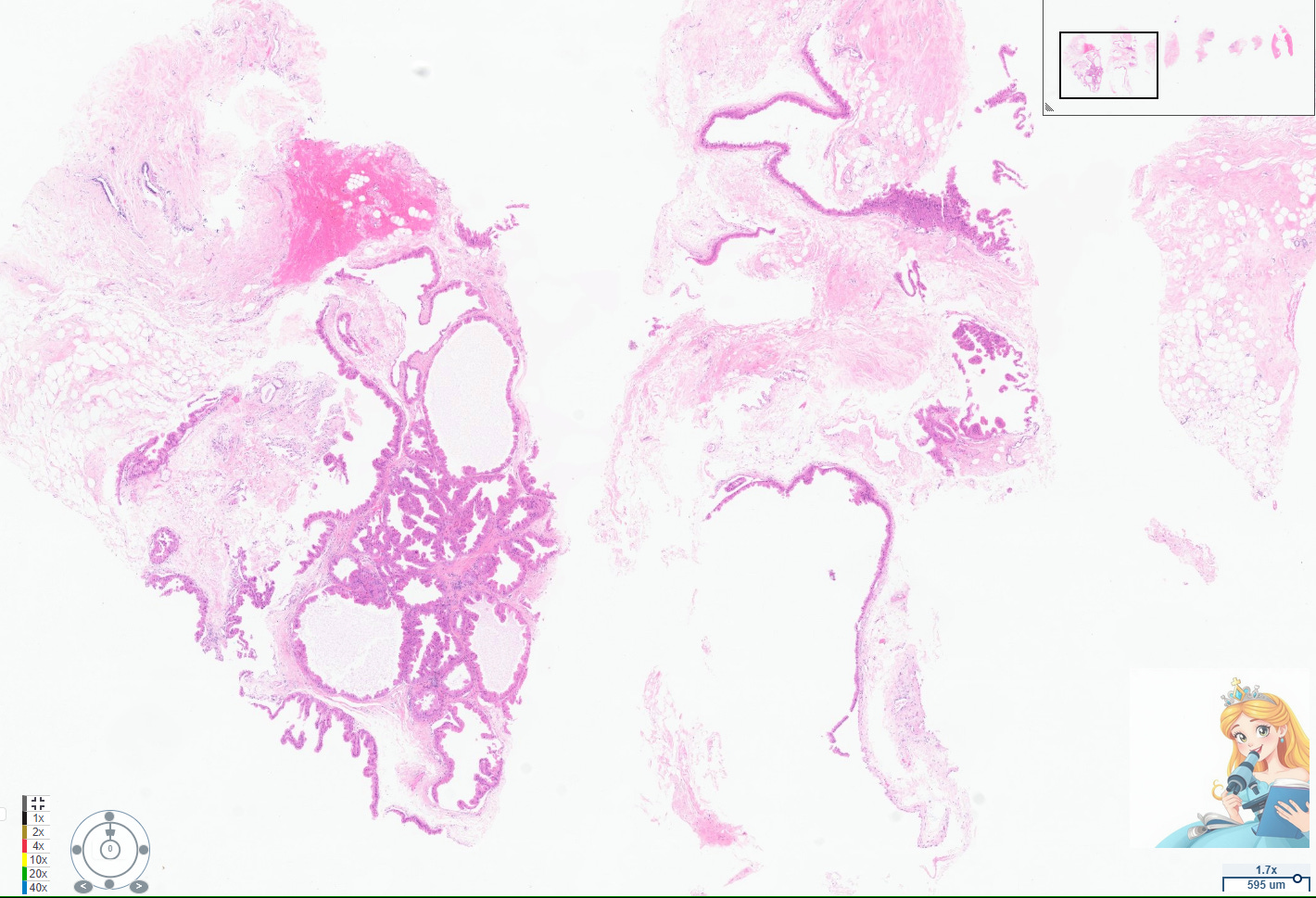
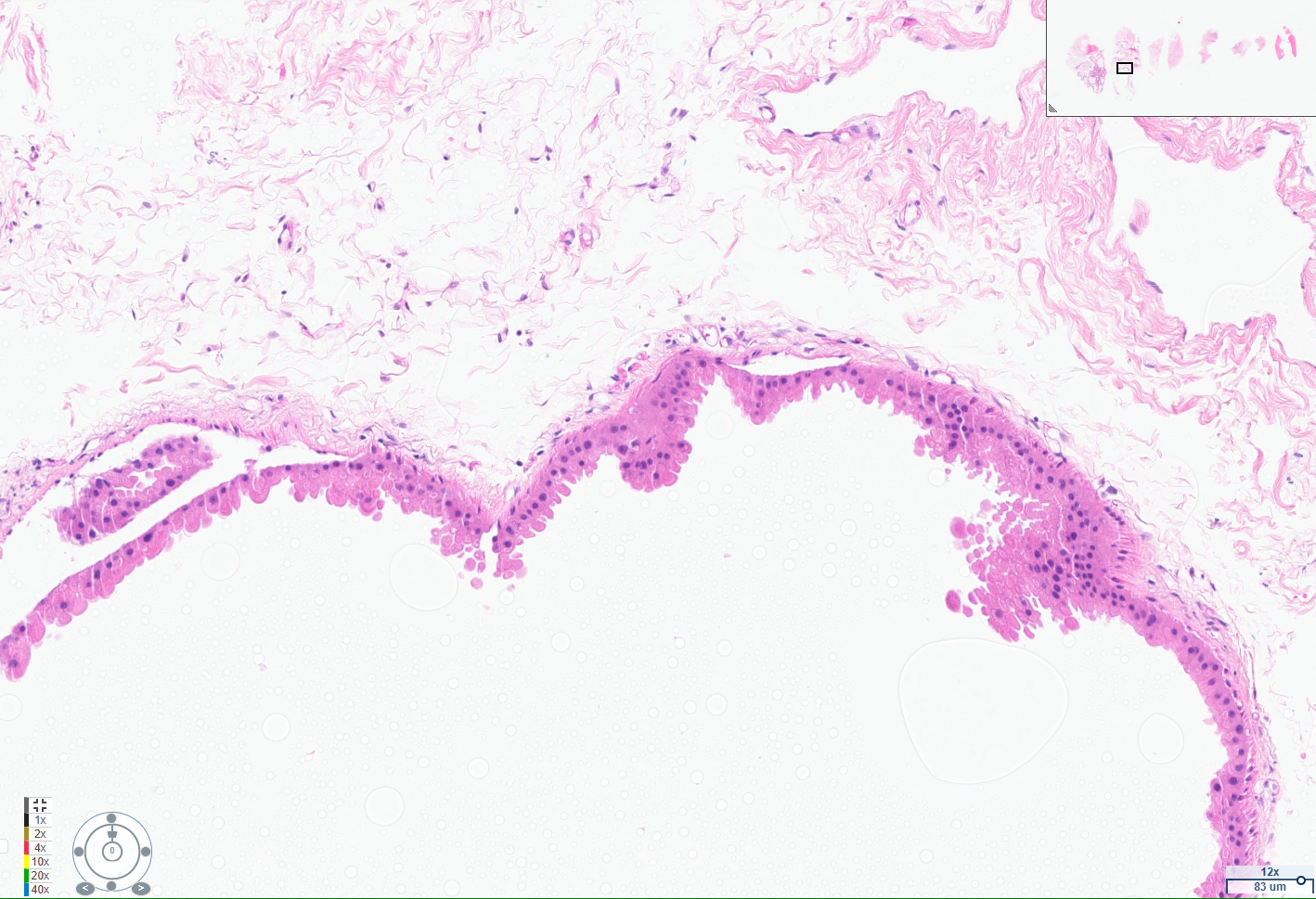
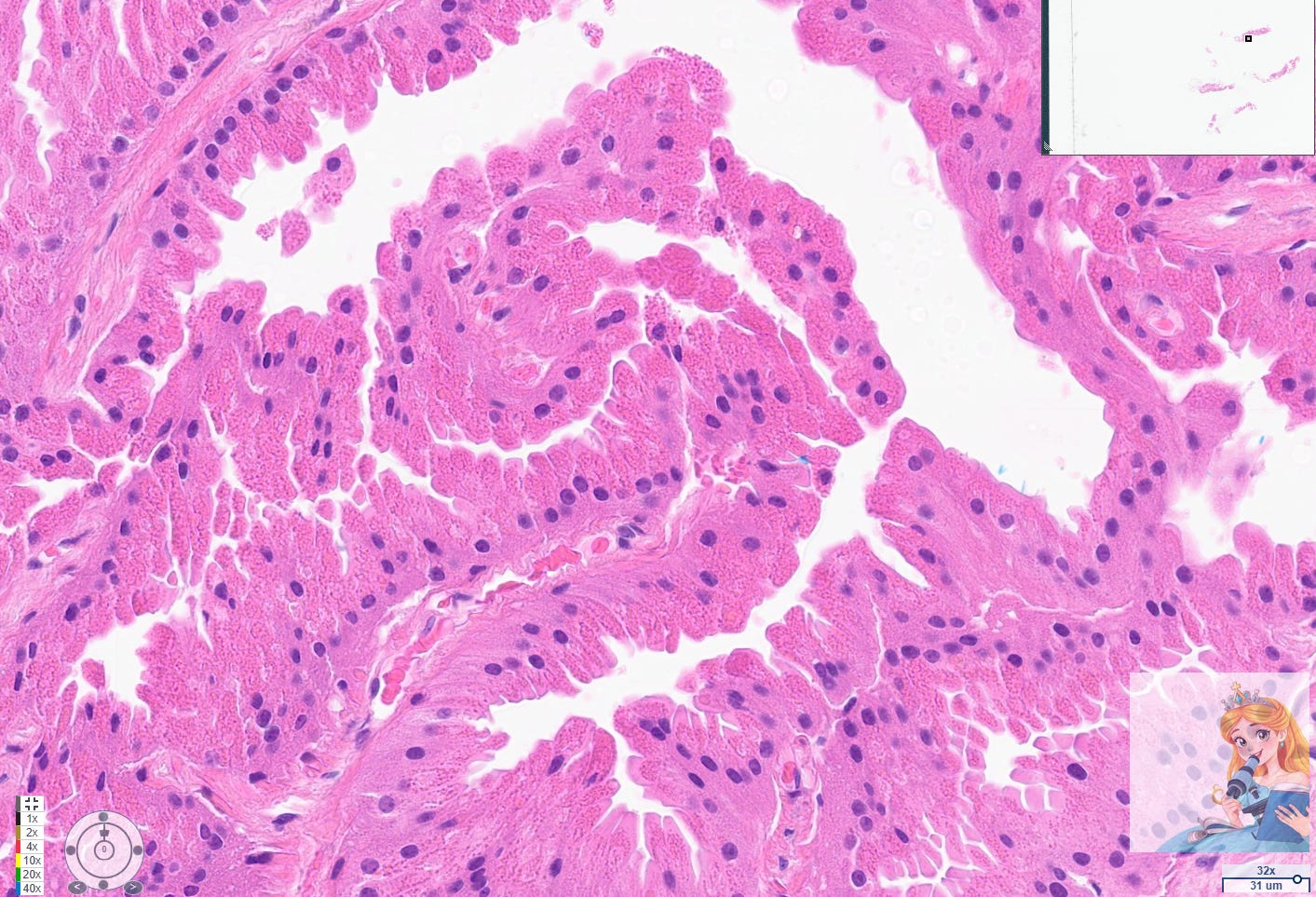
Apocrine cysts are a common manifestation of fibrocystic change in the breast, particularly in women over 25 years old. These cysts are lined by apocrine cells, which are characterized by abundant eosinophilic granular cytoplasm, round nuclei with pale chromatin, and prominent nucleoli. The apocrine lining may be cuboidal or columnar, and the cells typically have a low nuclear-to-cytoplasmic ratio and prominent apical snouts, reflecting apocrine secretion.[1-2]
Apocrine metaplasia is considered a benign, non-proliferative change and is frequently seen in the context of breast cysts, often as part of the broader spectrum of fibrocystic change. It is so prevalent after age 25 that it is regarded as a normal histologic finding in adult breast tissue.[2-3] The presence of apocrine metaplasia in cysts does not, by itself, confer an increased risk of malignancy, and these cysts are considered a hallmark of benign breast disease.[1-2][4]
Immunohistochemically, apocrine cells in these cysts consistently overexpress androgen receptor and lack estrogen and progesterone receptor expression, which can aid in their identification and distinction from other breast epithelial cells. It is rare that these stains need to be performed in daily practice. While some studies have explored the potential for apocrine metaplasia to be a precursor to malignancy, the overwhelming consensus is that cysts lined by apocrine cells with abundant eosinophilic cytoplasm and round nuclei are a benign and extremely common finding in women over 25 years old.[5][4]
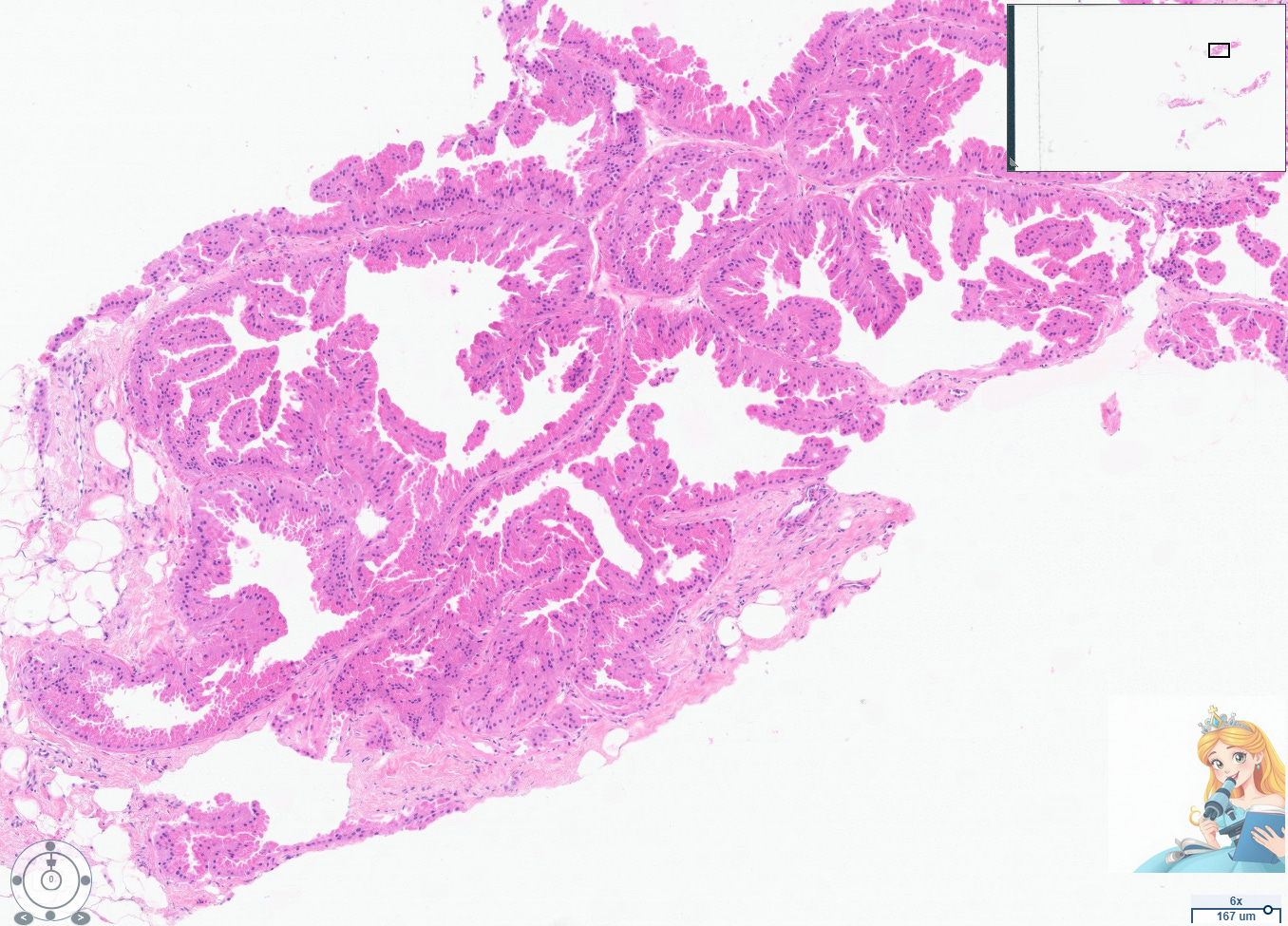
Abundant apocrine cystic change has been termed cystic papillary apocrine metaplasia by pathologists. However, using this term diagnostically can be confusing to radiologists who are concerned that the term “papillary” warrants consideration for excision. Always rule out a papilloma with apocrine changes when evaluating this particular type of apocrine changes, which can appear architecturally complex.
No specific treatment or follow-up is required for simple apocrine cysts unless there are atypical features or clinical symptoms.
Pearls of Wisdom:
Eosinophilic Cytoplasm + Bland Nuclei = Apocrine Change! This is your most reliable morphological indicator.
Common: Don't be surprised to see them; they're a part of benign breast life after age 25.
No Increased Risk: Simple apocrine cysts are benign and don't increase cancer risk.
No Specific Treatment: Unless there are atypical features or clinical symptoms, no specific treatment or follow-up is required.
Entry created in collaboration with AI tools.
References
Apocrine Lesions of the Breast: Part 1 of a Two-Part Review: Benign, Atypical and in Situ Apocrine Proliferations of the Breast. D'Arcy C, Quinn C. Journal of Clinical Pathology. 2019;72(1):1-6. doi:10.1136/jclinpath-2018-205484.
Non-Operative Breast Pathology: Apocrine Lesions. Wells CA, El-Ayat GA. Journal of Clinical Pathology. 2007;60(12):1313-20. doi:10.1136/jcp.2006.040626.
Apocrine Lesions of the Breast. Quinn CM, D'Arcy C, Wells C. Virchows Archiv : An International Journal of Pathology. 2022;480(1):177-189. doi:10.1007/s00428-021-03185-4.
The Histologic Spectrum of Apocrine Lesions of the Breast. Durham JR, Fechner RE. American Journal of Clinical Pathology. 2000;113(suppl_1):S3-18. doi:10.1309/7A2P-YMWJ-B1PD-UDN9.
Gatalica Z. Pathology, Research and Practice. 1997;193(11-12):753-8. doi:10.1016/S0344-0338(97)80053-2.