


Ductal Carcinoma in Situ (DCIS)
Breast Core Biopsy: DDX of Calcifications

Ductal Carcinoma In Situ (DCIS) is a non-invasive malignant proliferation of epithelial cells confined to the mammary ductal-lobular system, without evidence of invasion through the basement membrane. It is frequently detected on screening mammograms due to associated microcalcifications.
Histologic Features:
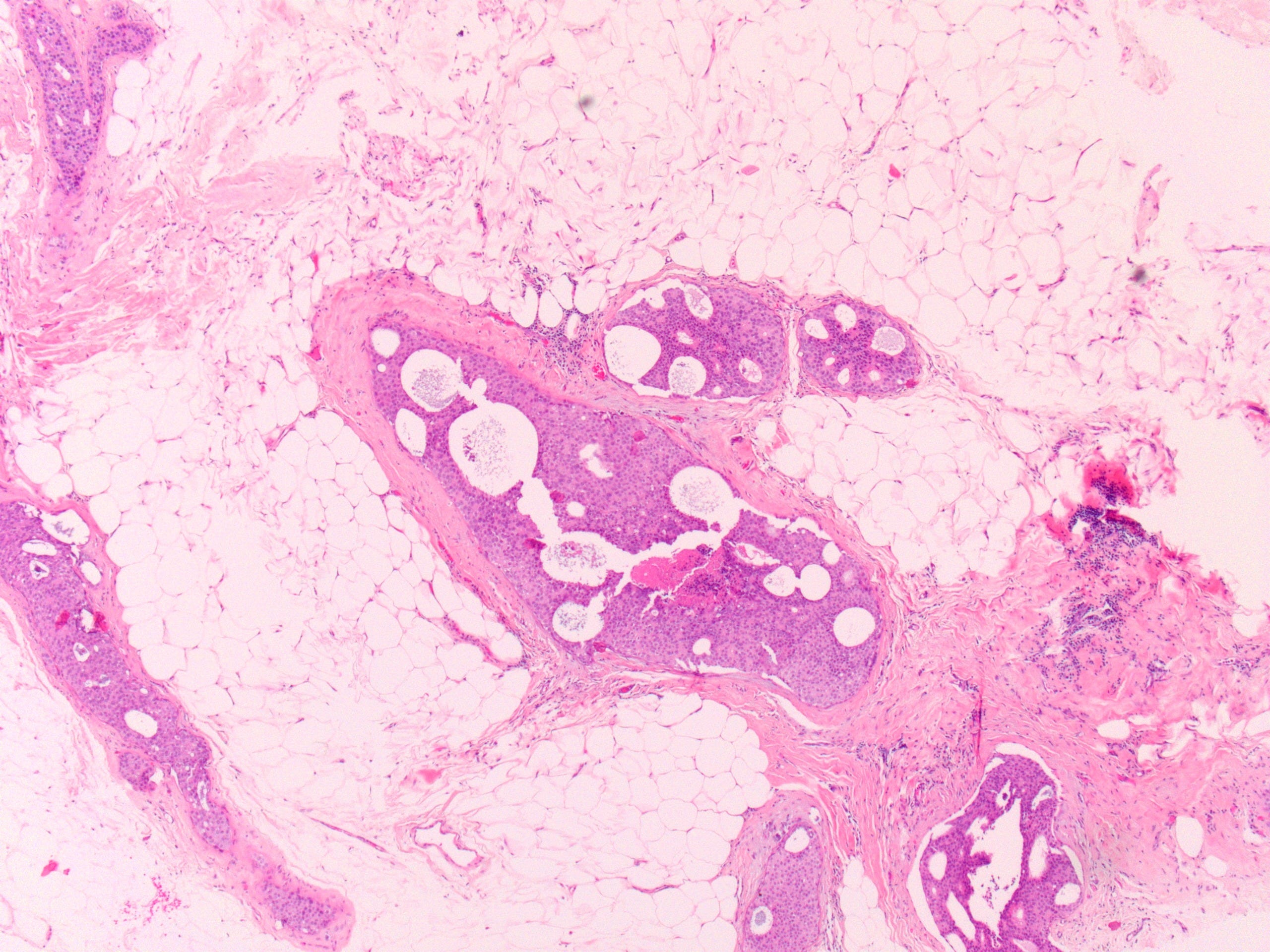
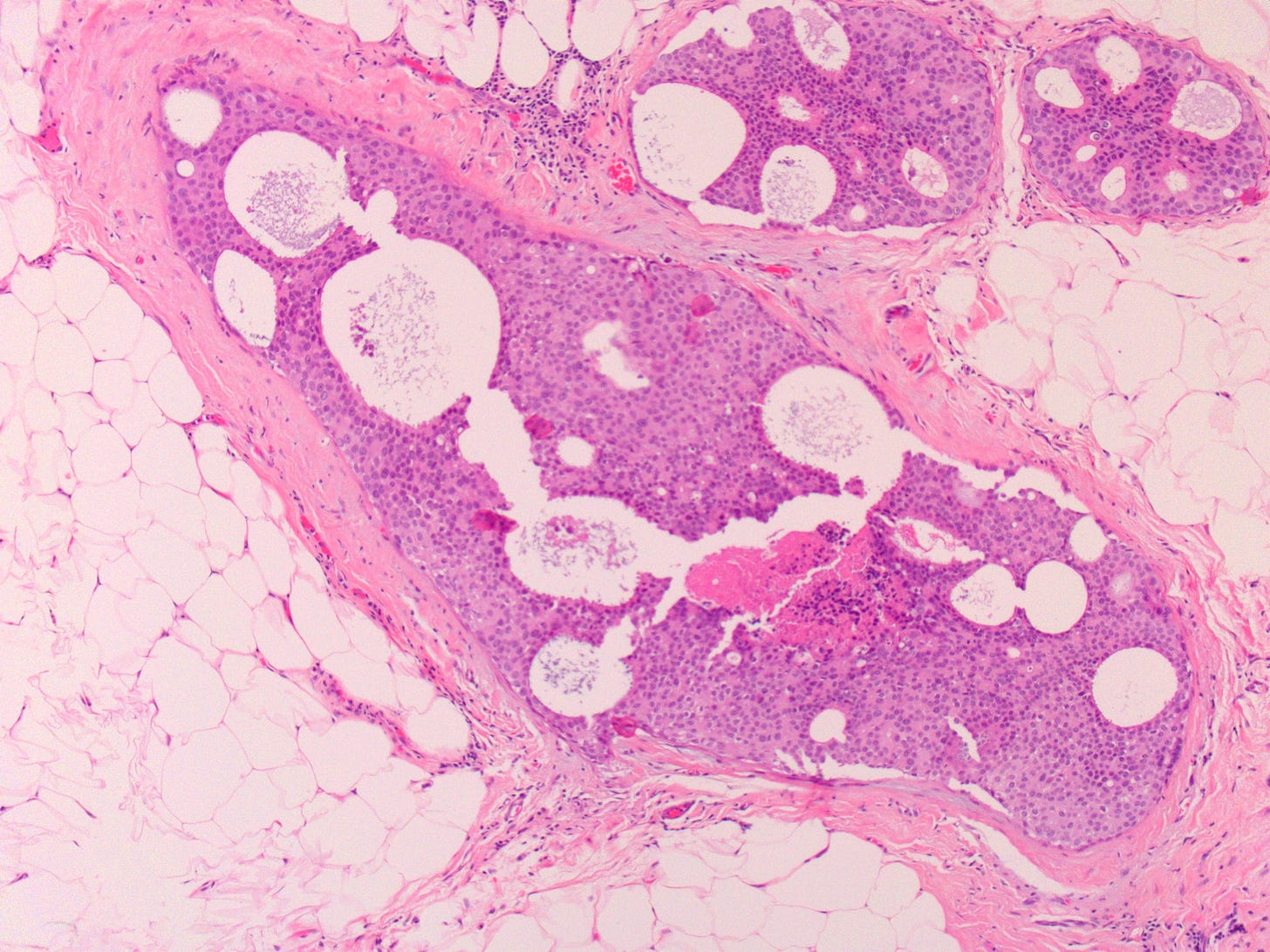
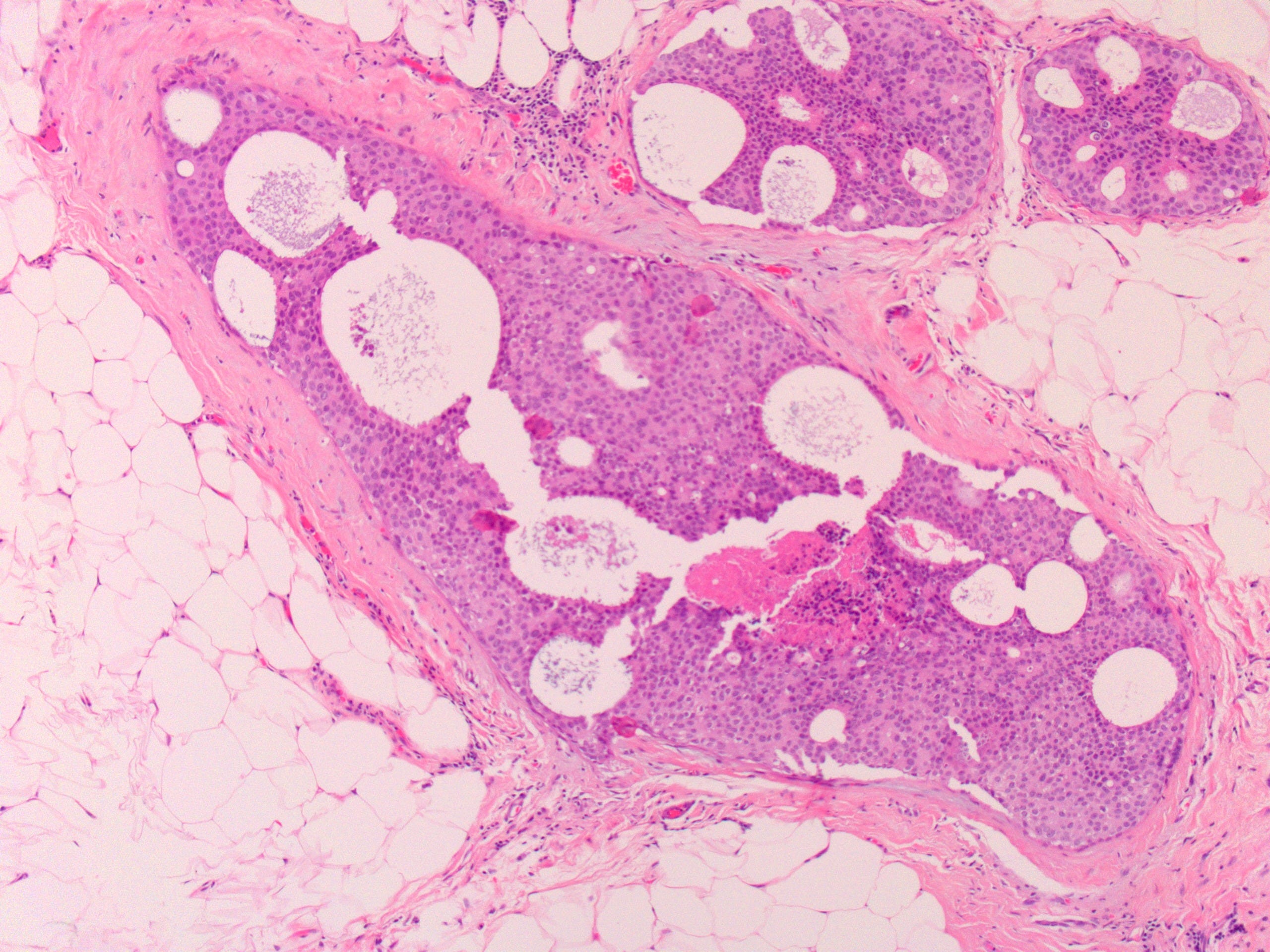
Malignant Epithelial Proliferation within Ducts: The defining feature is the presence of malignant epithelial cells completely contained within the lumen of the mammary ducts. These cells exhibit varying degrees of cytologic atypia and architectural patterns.
Architectural Patterns: DCIS is broadly classified by architectural patterns, often with mixed patterns present in a single lesion:
Comedo-type: Characterized by high-grade cytologic atypia (large, pleomorphic nuclei, prominent nucleoli, frequent mitoses) and central necrosis within the involved ducts.
Cribriform: Ducts are filled with a uniform population of cells forming "punched-out" or sieve-like spaces (pseudo-lumens).
Micropapillary: Cells form delicate, club-shaped tufts that project into the duct lumen without a fibrovascular core.
Papillary: Cells proliferate around true fibrovascular cores within the ducts.
Solid: Ducts are completely filled with a solid sheet of malignant cells.
Nuclear Grade: DCIS is also categorized by nuclear grade (low, intermediate, high), reflecting the degree of cellular atypia and mitotic activity. High-grade DCIS (often comedo-type) typically shows larger, more pleomorphic nuclei, prominent nucleoli, and necrosis.
Intact Myoepithelial Layer: Crucially, the myoepithelial cell layer, located between the malignant epithelial cells and the basement membrane, is preserved in DCIS. This distinguishes it from invasive carcinoma.
Calcifications:
Location: Calcifications in DCIS are typically intraluminal, forming within the necrotic debris (in comedo-type DCIS) or secretions within the ductal lumens.
Morphology on Histology: On hematoxylin and eosin (H&E) staining, DCIS-associated calcifications appear as basophilic (purplish) deposits. Their morphology can vary:
Amorphous/Granular: Small, indistinct, powdery, or cloudy calcifications, often seen in non-comedo DCIS.
Fine Linear/Branching (Casting): These calcifications are highly suspicious for malignancy and often correspond to the necrotic material within the lumens of involved ducts, taking on the shape of the duct. This type is particularly associated with high-grade, comedo-type DCIS.
Laminated/Crystalline: More regular, sometimes concentric or crystalline structures, often found in low-grade DCIS.
Mammographic Correlation: The presence, morphology (e.g., fine linear branching, fine pleomorphic), and distribution (e.g., clustered, segmental, linear) of microcalcifications on mammography are key indicators for DCIS, necessitating biopsy. Histologic examination of the calcifications confirms that the mammographically targeted area was adequately sampled.
Significance:
DCIS is a non-obligate precursor to invasive breast cancer. While it does not metastasize, it carries a risk of progression to invasive disease if untreated. The presence of calcifications is often the only clinical manifestation, making their accurate assessment critical for early diagnosis and management. The type and extent of DCIS, particularly nuclear grade, have implications for prognosis and treatment planning.
This post was created in collaboration with AI tools